

https://www.shrinershospitalsforchildren.org/st-louis/halo-traction
Earlier this spring I put up three blog posts on Halo-Gravity Traction. I will briefly re-present it here as a way to launch into the two other types of traction we utilize: Intraoperative Halo-Femoral Traction and Internal “Dis-traction” Technique.
What is
halo-gravity traction?
As you see from the
three young patients above, a “halo” is applied to their skulls when they are
asleep in the operating rooms. On the
two boys their halos are black, as they are made from carbon fiber, while the
young lady’s halo is so nicely bedazzled you don’t see any of the black carbon
fiber material. Attached to the halo you see two straps or an inverted-V which
is then attached to a rope which is pulling upwards, towards the ceiling.

The rope goes
through a series of pulleys and finally attach to weights.
Why do we put
patients into halo-gravity traction?
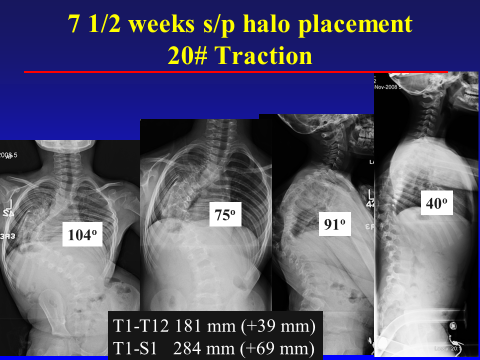
The below case is
a nice example of why we use halo-gravity traction, a 5 year old female with
severe early-onset scoliosis at 104 degrees (picture on left) and 91 degrees of
kyphosis (2nd picture from right). After 7 weeks of traction the scoliosis
decreased to 75 degrees (a 28% improvement!) (2nd picture from left)
and 40 degrees (a 57% improvement) of kyphosis (picture on right). Overall there was an 80 degree improvement in
the spinal deformity! This was all done only with halo-gravity traction, and no
spine surgery.
In general, we apply preoperative traction for any
severe spinal deformities, which can be curves greater than 90 degrees.
How does it work?
Spinal traction
takes advantage of the viscoelastic properties of the spinal column. Think of the
spine like a spring, a person with scoliosis would be the spring on the far
left, crooked/twisted and very short from the top of the spring to the bottom
of the spring. As we apply more and more
weight to the spine, the curves straighten out and the spine gets longer. In the case demonstrated above the spine
lengthened (from the bottom of the neck to the pelvis) a total of 69 mm or 2.7
inches!

However there is
a limit to how much weight we can safely put through the traction
apparatus. This maximal limit varies
patient to patient but we typically don’t go higher than 50% of the patient’s
body weight.
In next blog post we will demonstrate another type of traction: Intraoperative Halo-Femoral Traction