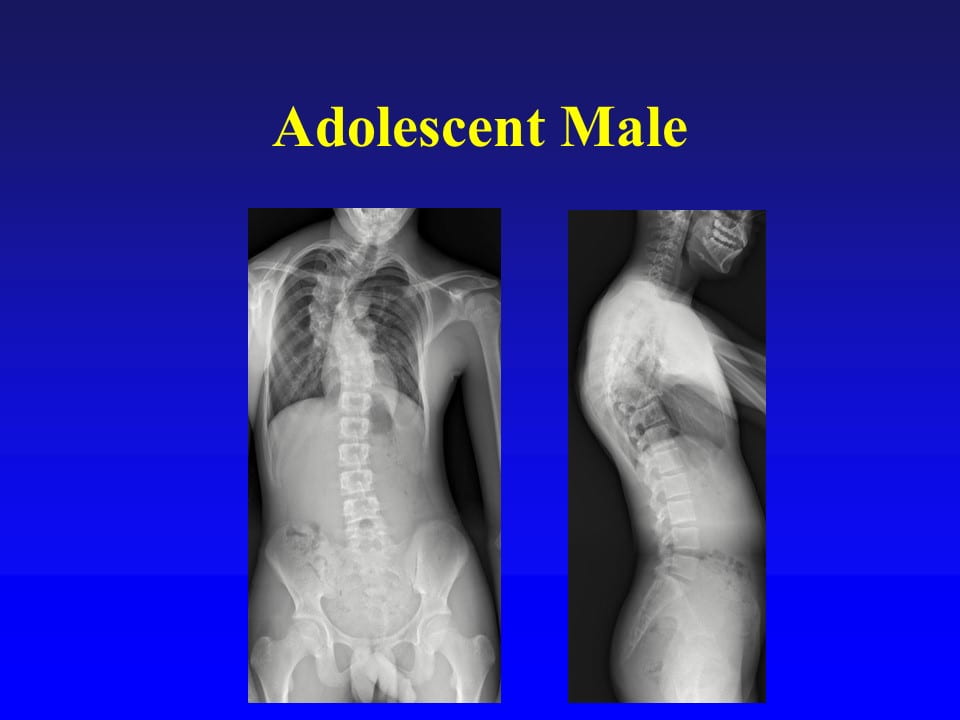
The case presented in this blog is an adolescent male, who is an active athlete and having back pain. It is easy to see the scoliosis in the upper part of the spine.
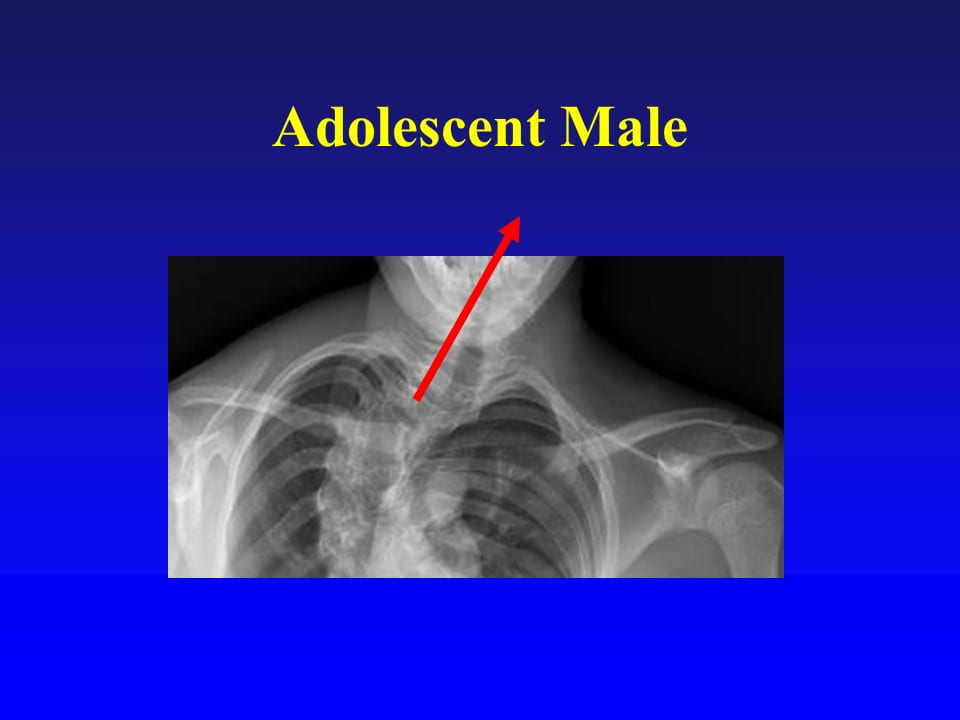
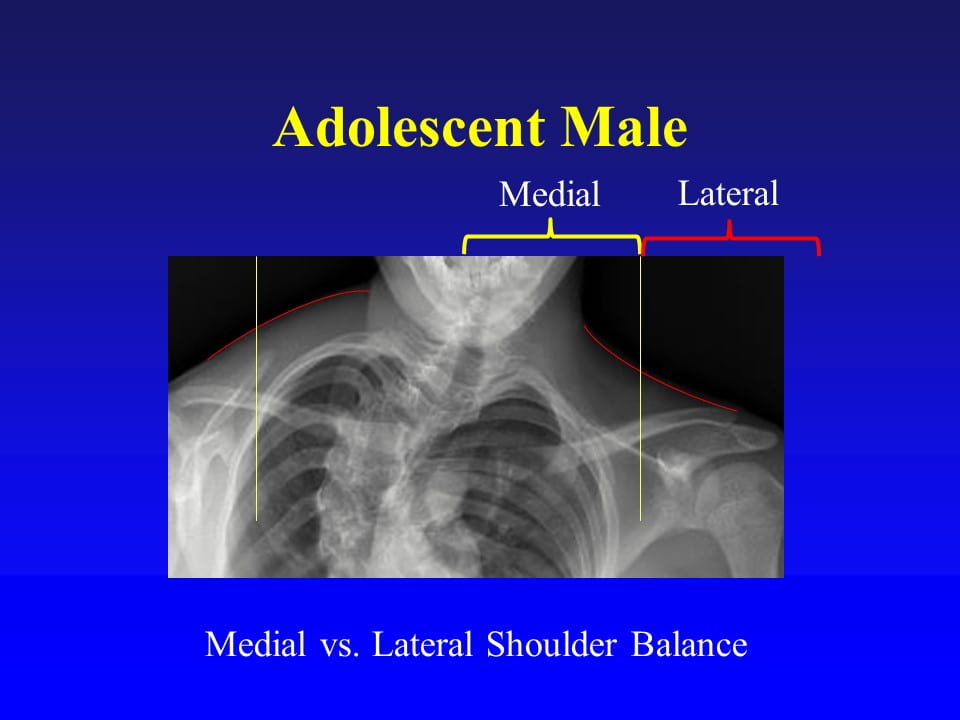
The below picture demonstrates the impact of scoliosis on the shoulder and neck alignment. Due to the scoliosis which tips the head to the right (see red arrow).
Despite the presence of the shoulders (see green line), the neck contour is very asymmetric (red curve lines). On the left the neck contour is CONVEX, whereas the right neck contour is CONCAVE. This occurs due the tipping of the neck to right, and because the scoliosis causes the ribs to rotate backwards on the left which creates the convexity of the neck.
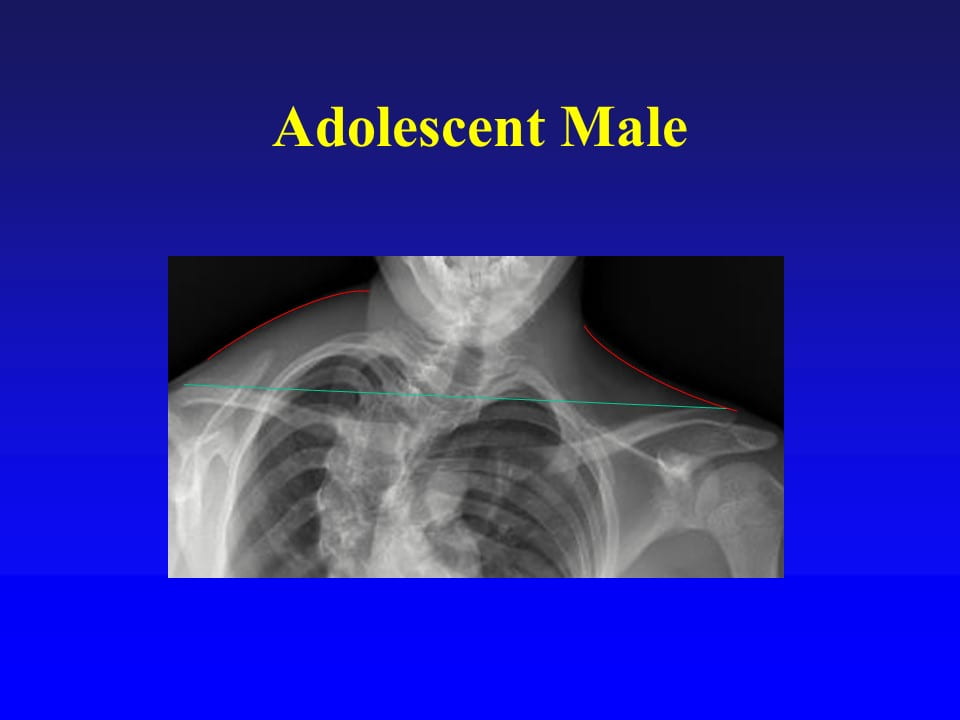
The region of the shoulders can be broken down into the medial and lateral shoulder balance. The lateral shoulder balance is really how high the actual shoulder joints are relative to each other. The medial shoulder balance is what we just called the neck contour.
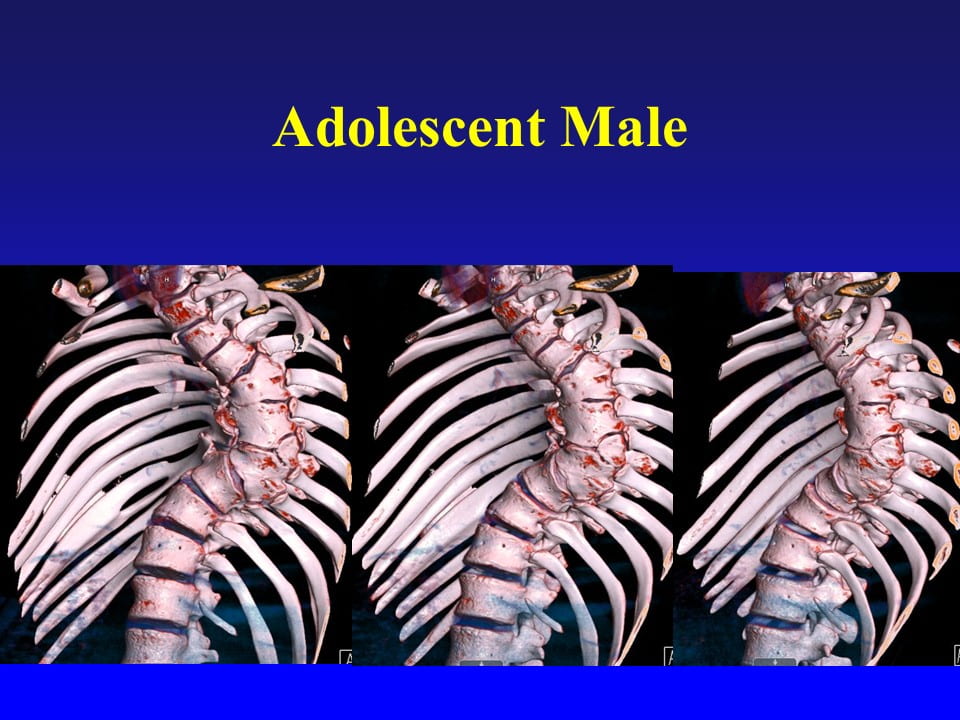
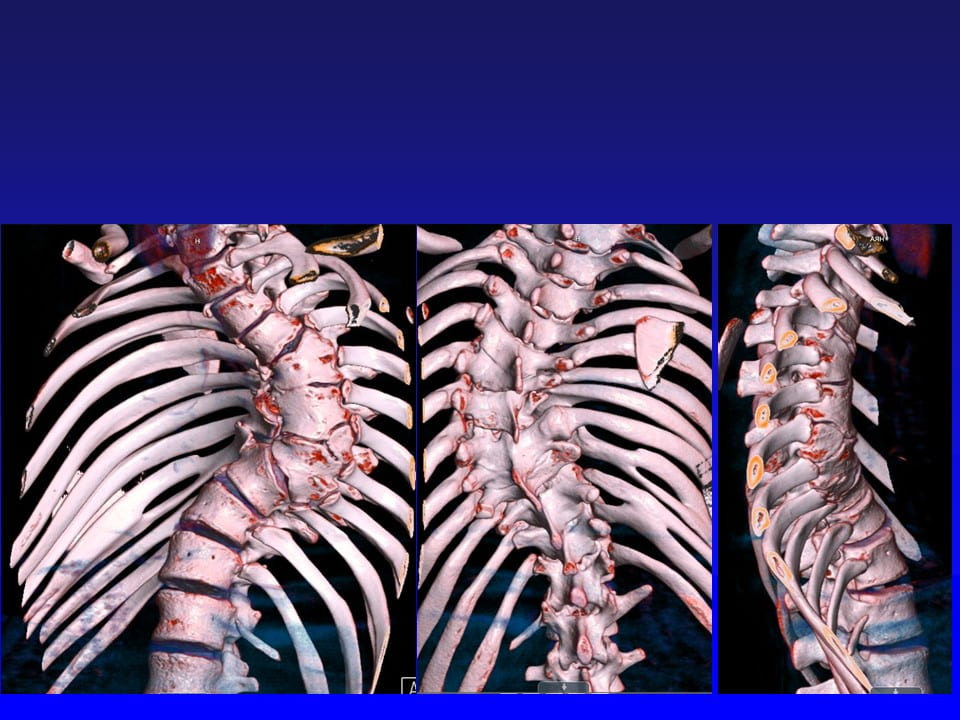
The next two slides are 3-dimensional CT scan reconstructions of this patient’s deformity. These images nicely demonstrates that there are partially-formed vertebra and other vertebra are partially fused. The presence of both failure of formation and failure of segmentation vertebra make the diagnosis of this type of congenital scoliosis as “Mixed-Type”.
The 4 radiographs below demonstrate the scoliosis and spine are stiff, meaning they don’t move much with bending or pushing on the spine.
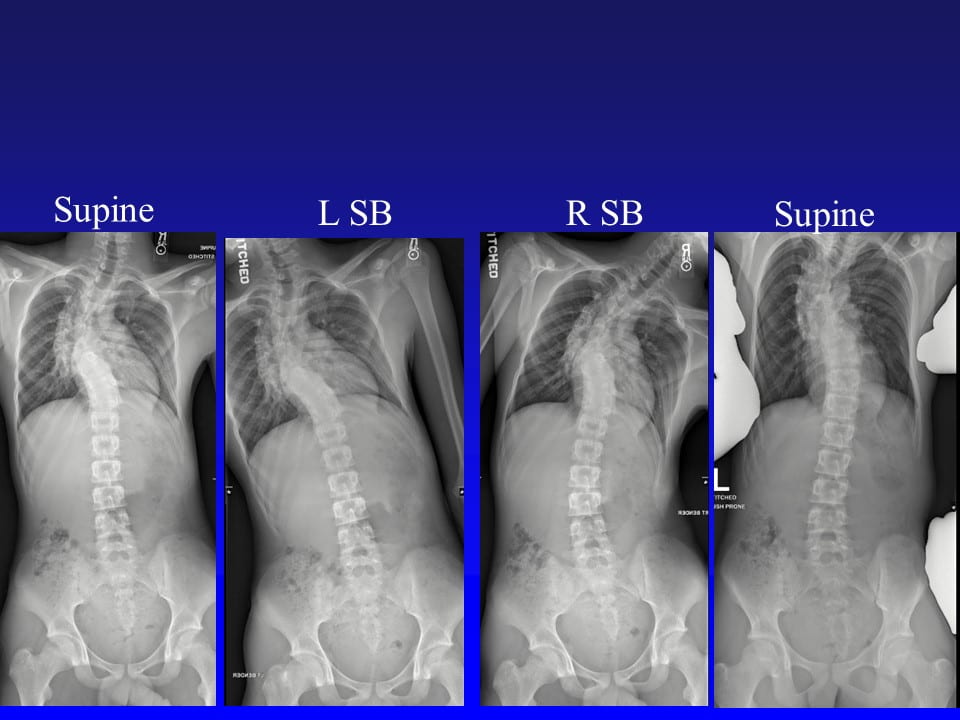
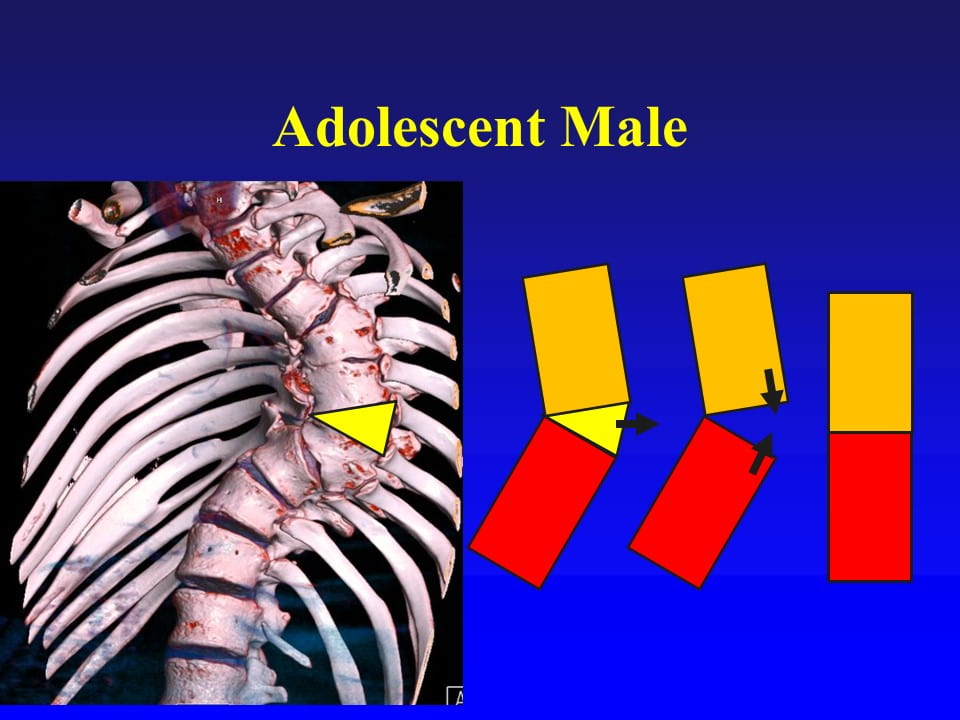
So we have an adolescent male has a severe, mixed-type of congenital scoliosis. The next step is to decide how to reconstruct the spine. Because the spine is stiff we cannot do the usual type of surgery, which is to put in screw and then bend the spine straight. This spine will not bend, so we will need to resect a part of the spine, taking a wedge out of the spine

The technique is to drill out (remove) a triangular, wedge-shaped part of the spine (yellow triangle), creating a gap in the spine. This gap is then closed down to straighten the spine.
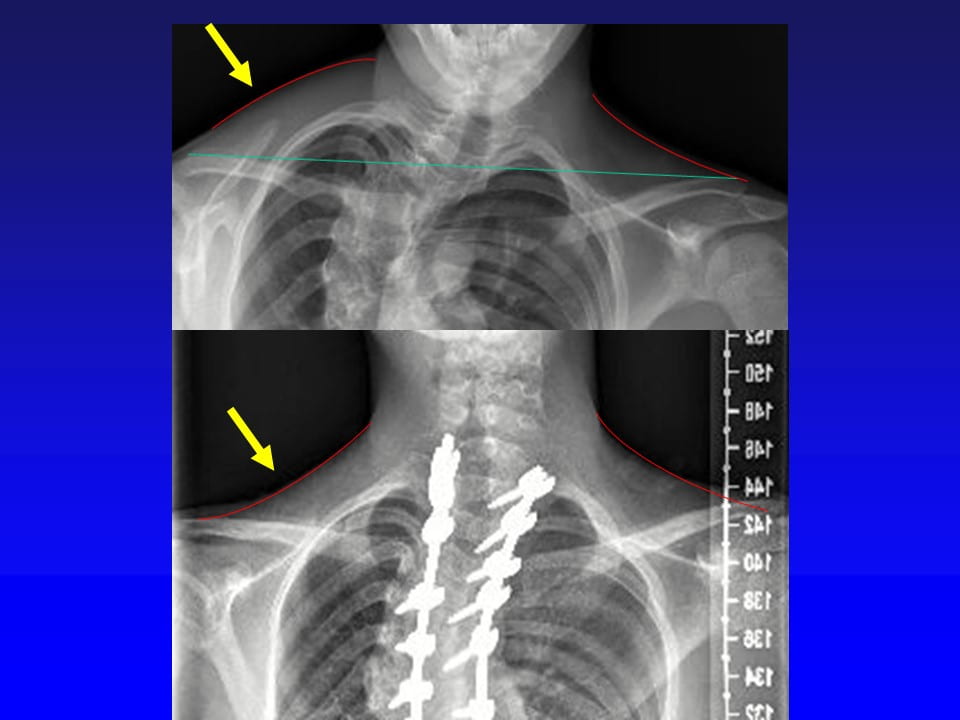
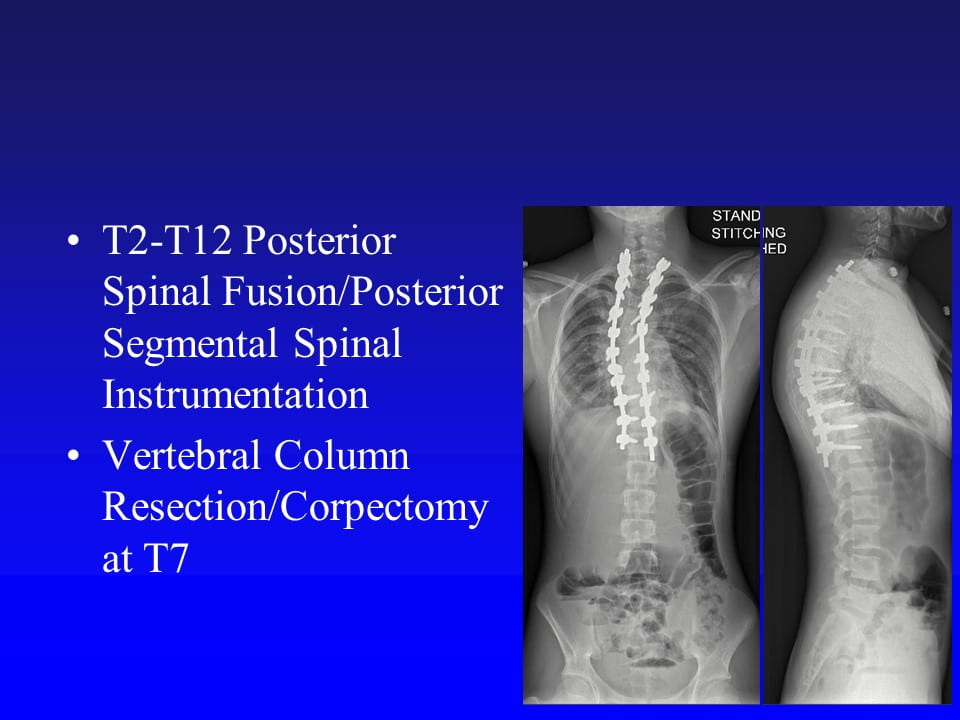
Surgery was performed with a posterior spinal fusion from T2-T12 and by resecting (called a Vertebral Column Resection or Corpectomy) the very abnormal T7 vertebra in a wedge-shape then closing the gap down to straighten the spine.
It is easy to see how much the spine improved both from the front and the side views.
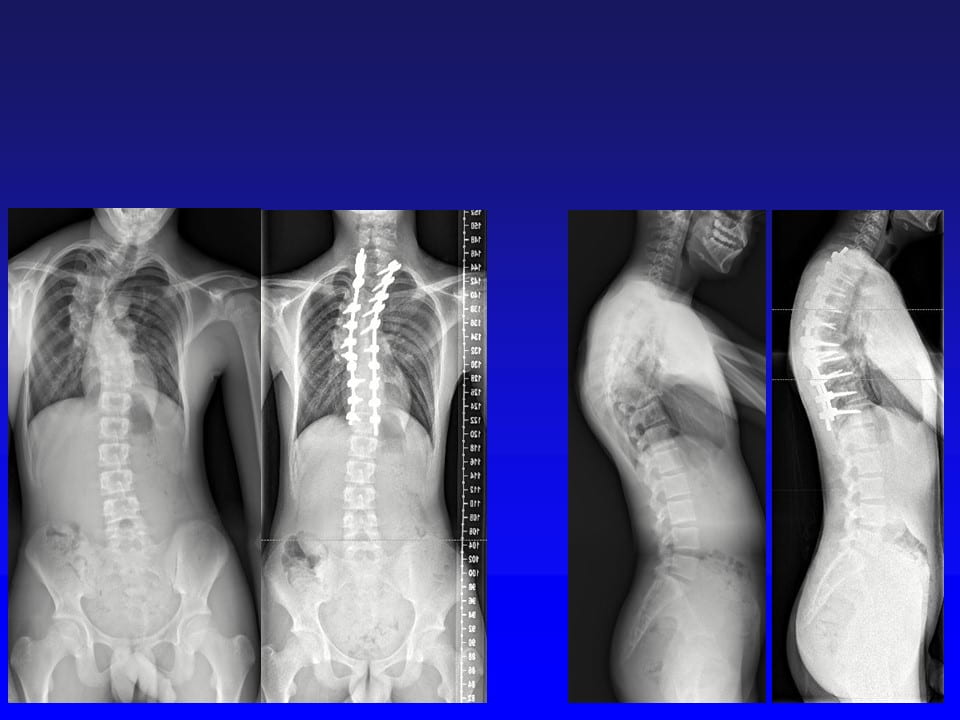
If we look specifically at the medial shoulder alignment or neck contour, you can see how the left and right side are almost perfectly equal!
Safely performed a vertebral column resection (VCR) or corpectomy is a powerful procedure in correcting spinal deformity. However, it is important to remember this type of surgery, on this type of patient, has higher risks of spinal cord problems than other diagnoses and surgeries. The use of a VCR should only be performed at high-volume pediatric spine deformity centers to optimally perform the surgery.