As previously mentioned congenital scoliosis comes in a wide
range of types, locations, and complexity.
This means surgeons caring for this group of patients needs
to have multiple surgical
treatment options to optimally care for this potentially challenging
deformities, from simple hemivertebra resections to complex vertebral column
resections and Shilla constructs. The below three cases demonstrate the
progression from simple to complex, both in terms of the deformity and the
required surgery.
Simple: 7 year old male with a single hemivertebra
treated with resection and short fusion



Moderate: 13 year old female with previously operated
(outside hospital) on lumbosacral hemivertebra with continued worsening of
deformity. Underwent hemivertebra
resection and longer fusion.



Complex: 8 year old male with Prune Belly syndrome. Treated with vertebral column resection (VCR)
at T10, and Shilla construct T4-L4.



On the more complicated end of the congenital scoliosis
spectrum (i.e. mixed-type), the simple resection and short fusion may not be
the best option. This is due to the
possible presence of adjacent areas of involvement which may induce increasing
curves above or below the surgical site.
In the past if this was a concern after surgery, the patient may be
placed into a brace, which often is less than ideal as these patients may need
to wear a brace for many, many years.
Shilla treatment of congenital scoliosis
The “complex” case above was treated with a VCR and a Shilla
procedure. However performing a Shilla
procedure in less severe cases can be optimal.
The below case is a 4 year old male with two areas of congenital
deformity (one higher and 31.5 degrees, and one lower and 46.8 degrees).
CASE 1

Because of the upper deformity was congenital and more stiff
(see below slide), a simple hemivertebra resection will not be able to control
the upper curve.

So, at the time of surgery the left T10 hemivertebra (the
lower curve) underwent a VCR (complete removal of the vertebra), and then
Shilla T4-L4

The arrow on the below slide shows the closure of the gap
when the T10 hemivertebra was resected.

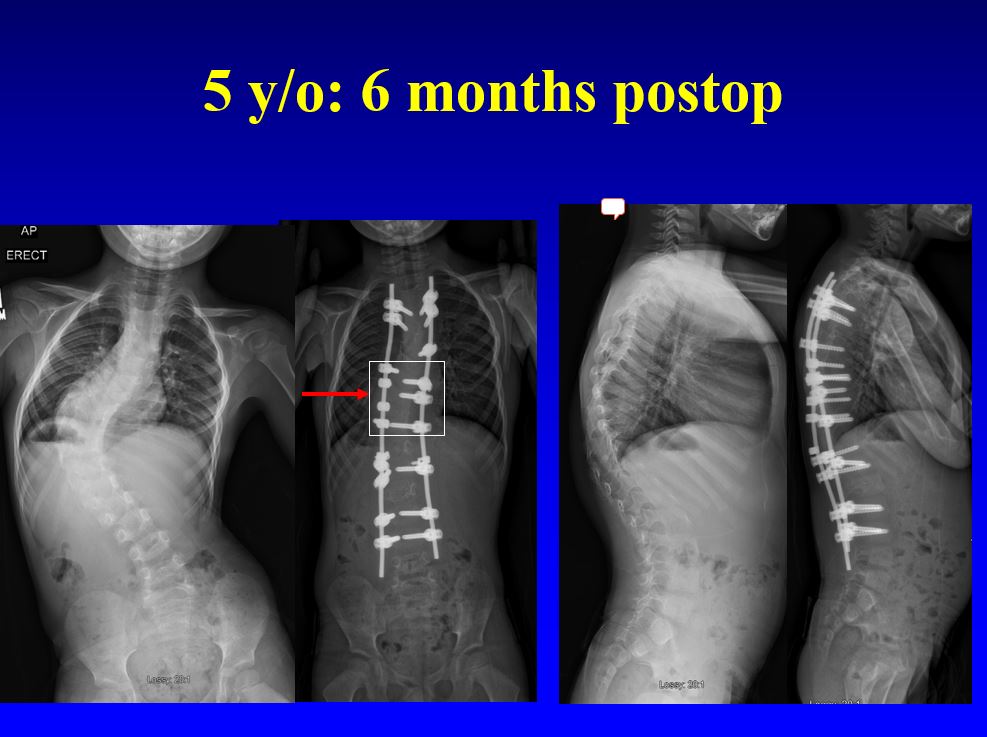
Here is the 6 months after surgery follow-up. His body shift to the left is significantly
improved. The only levels of fusion are
within the white box (below). The
remaining vertebra above and below this white boxed area will be able to grow
vertically along the Shilla rods.
The next Blog post
will demonstrate complex congenital scoliosis cases using Shilla procedures