In the previous blog post, we presented “what is a spine fusion”?
In most pediatric spine surgeries metal implants correct and
stabilize the spine in a new position (see below), then a spine fusion is
performed.


What I tell families/patients: “The metal allows us to
attain and maintain the spine in a new position while the spine then creates a
bony fusion”
How do you get a spine to fuse? During surgery, after the
implants are placed and the spine is corrected (see above), the fusion part of
the surgery is then done. This involves decorticating, or roughening up, the
bone in the back of the spine. This stimulates
the bone to heal, and the bone graft then is laid over this roughened
bone. The body breaks down, or digests
this new bone graft and then creates a solid bony connection.
In the past, we used to always use the patients’ own bone,
usually taken from the iliac crests above the hip joints. This type of bone is
call “Auto-graft” = the patient’s own bone, whether it be from the spine,
pelvis or both.
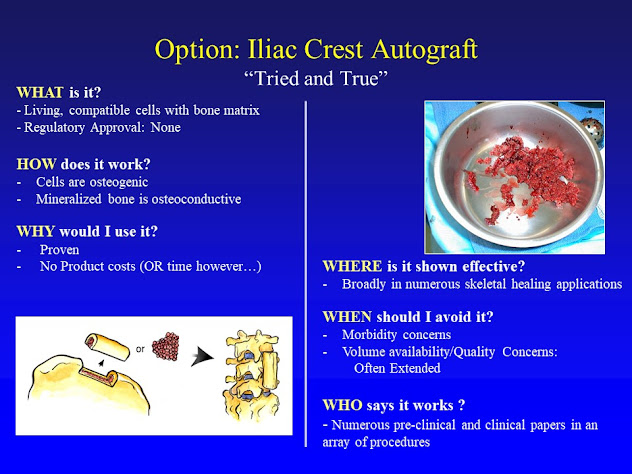
Harvesting the iliac crest bone takes additional time in the
OR and it really hurts after surgery.
Since we have switched to allograft the amount of postoperative
narcotics needed and the length of time patients’ were having significant pain
has declined.
The standard of care now in pediatric spine surgery is to
use allograft bone. “Allo-graft” =
another person’s bone.
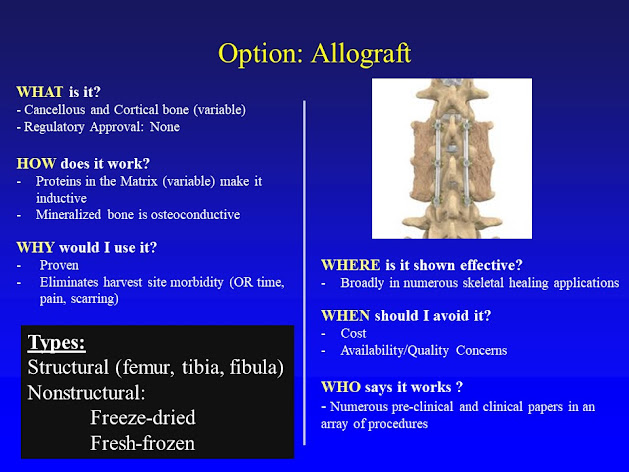
Bone is not rejected from the person receiving it, unlike in
other type of tissue transfers between people.
There are no antigens on bone, unlike other transplanted tissue such as hearts
or livers.
At present, during spine surgery there is some small amount of
the autograft, or the patient’s own bone, which is collected during surgery,
but the majority of the bone used is allograft.
So both types are used in deformity surgery, but most of the volume is
because of allograft.