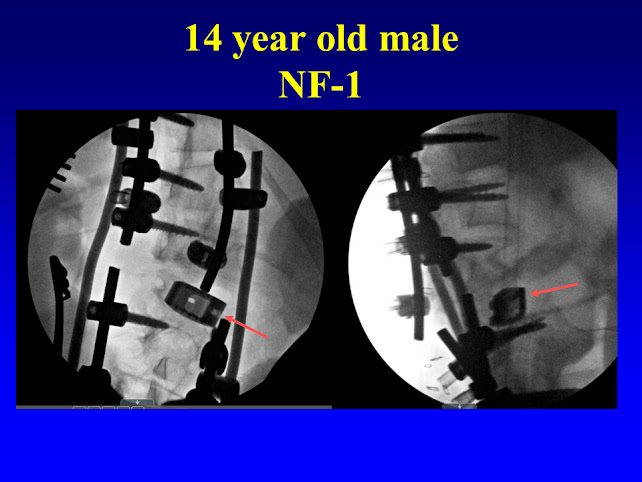
Surgical Case #2
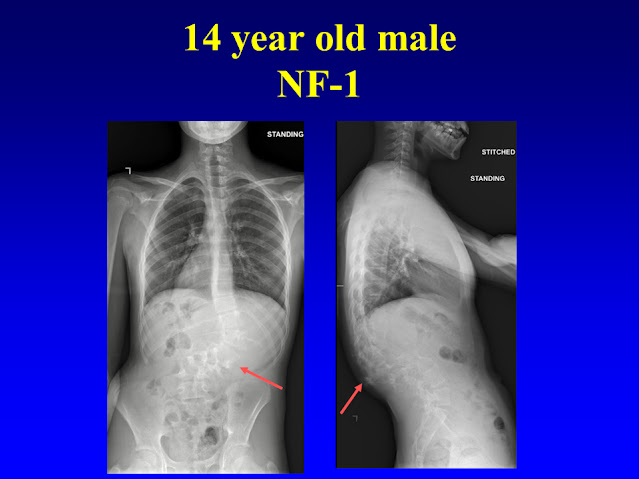
case is a 14 year old male with NF-1.
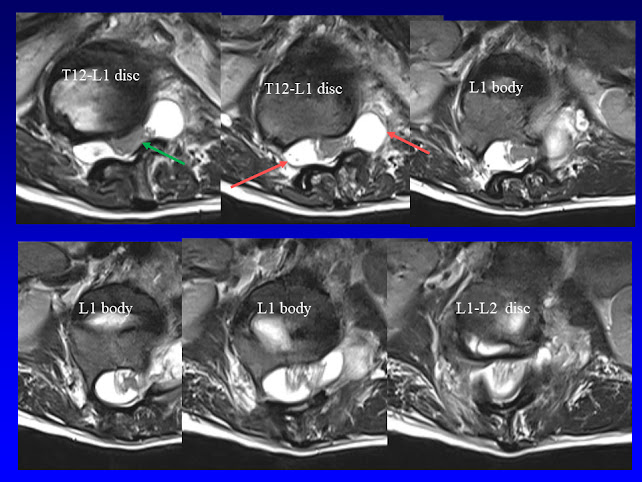
There are dystrophic changes to the spine around the thoracolumbar
junction, specifically penciling of the ribs and scalloping of the vertebral
bodies (red arrows). This has induced a
painful kyphoscoliosis.
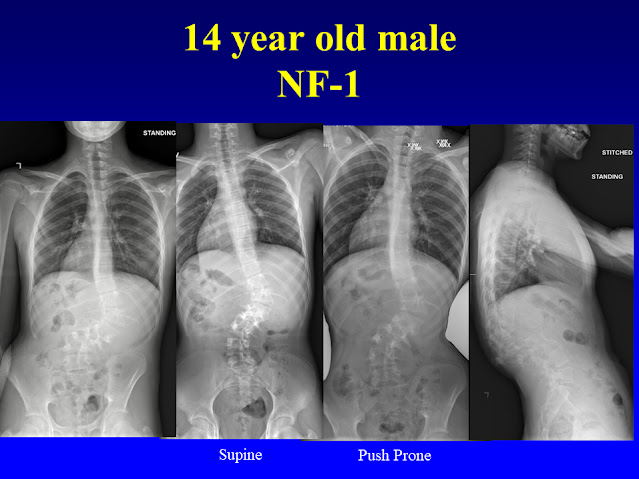
The next
pictures demonstrate there is some, but not much flexibility of the spine
deformity. The second picture from the
left is a supine (laying on one’s back) radiograph. The third from the left is a push-prone
(laying on one’e stomach and radiology technicians pushing to try to improve
the spine deformity. Neither of these two do much to change the spine deformity
position.
The below
two radiographs are performed with the patient actively bending to the left and
right.

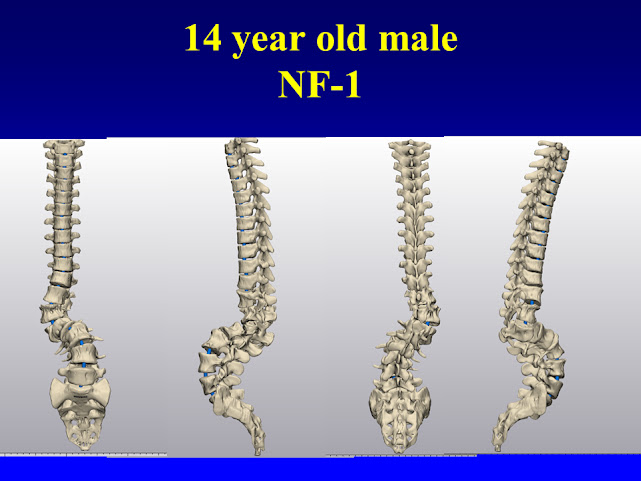
The below
pictures are made from a CT scan, which is then rendered into a 3-dimensional
picture which one can rotate around to better understand the deformity. These particular images were made just prior
to the creation of a 3-d model.
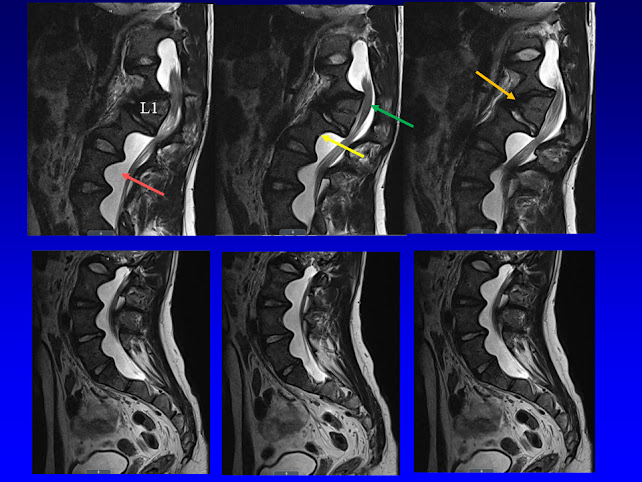
The below
MRI images demonstrates dural ectasias (red arrows), vertebral scalloping
(yellow arrows), and wedging of the vertebra (orange arrow). The spinal cord (green arrow) is bent
around the backside of the L1 vertebra.
The next
pictures are intraoperative radiographs (x-rays). Fixation of the spine can be very difficult
(due to dural ectasias and vertebral scalloping) and the quality of the bone to
be softer than normal (osteopenia).
Spinal deformity surgery of NF-1 patients requires preoperative CT and
MRI evaluations to understand spines and where fixation could be placed and how
to correct the spine deformity. Surgery
typically requires use of screws, hooks and sublaminar bands to successfully
treat NF-1 spines.
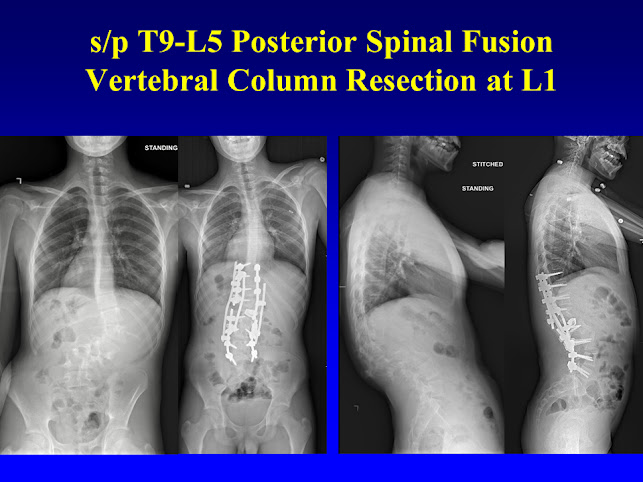
After the L1
vertebra was completely (100%) removed a titanium cage (red arrow) was placed
between the vertebra above (T12) and below (L2). This cage increases the strength of the spine
construct.
Below are
the before and after surgery pictures.
The surgery nicely improves the spinal alignment on both views. There was no weakness or sensory changes
after surgery. The patient’s
preoperative pain resolved.
Multiple
rods across the area where L1 was resected, and the cage was placed, to add
more rigidity and durability.