

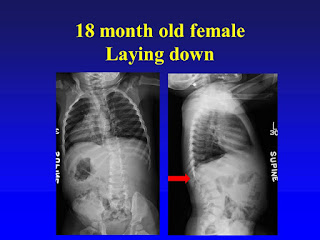
She was moving her legs normally and was felt to have normal
sensation in her legs. The red arrow
points to the T12 vertebra which does not sit under the T11 vertebra (orange
arrow).
The right side X-ray shows how the upper spine (thick green
line) does not line up with the lower spine (thick red line)

When lying down the T12 vertebra does not move under the T11
vertebra…..it is dislocated.
On the below CT scan cuts the red arrows point to the
dislocation, with T12 sitting too far back.

The below MRI cut nicely shows how the spinal cord is draped
over the posterior T12 vertebra. It is
easy to see if the dislocation gets worse the spinal cord will get more
compressed and deformed, which would then cause problems with muscle function
and sensation in the legs and cause bowel and bladder incontinence (inability
to control).

To correct the dislocation, the T12 vertebra needed to be
completely removed, and once it was the spine was very mobile and allows T11
get appropriately lined up with the L1 vertebra. Because there was a space between T11 and L1
a cage (yellow arrows) was put between them to add to stability and put the
spinal cord at the correct length.
Four pedicle screws were placed above and below the removed
T12 vertebra and were locked down. To
make sure this area heals solidly, and permanently a bone graft was placed in
the cage in the front and also in the back of the spine.

In the below slide the patient is now 6 weeks after
surgery. It is easy to see the
improvement of the spine alignment back to normal. Because the bone is soft at this age we kept her
in a brace for 6 months to protect the surgery.

Here she is now 8 year out after surgery. She has normal spinal alignment and normal
function of her spinal cord. Her
long-term prognosis is for a normal life.
