My first on this surgical technique was in August of 2018,
and I posted yesterday how I compare Shilla Growth Guidance against Traditional
Growing Rods and MAGEC Growing Rods. I
will continue to discuss the Shilla Growth Guidance System using a
Frequently-Asked-Question format, based on questions parents and caregivers have
asked me over the last 10 years.
and I posted yesterday how I compare Shilla Growth Guidance against Traditional
Growing Rods and MAGEC Growing Rods. I
will continue to discuss the Shilla Growth Guidance System using a
Frequently-Asked-Question format, based on questions parents and caregivers have
asked me over the last 10 years.
What size of scoliosis curve can be treated with a Shilla?
The Shilla Growth Guidance System has been used in the treatment
of scoliosis 40° or greater (up to 115°, typically 60-80° range).
of scoliosis 40° or greater (up to 115°, typically 60-80° range).
Can Shilla be used in patients at or near skeletal
maturity?
maturity?
This Growth Guidance System requires the patient have spinal
growth remaining to justify the modulation or guidance of spine growth. In general, we perform this surgery in patients
where spinal growth is anticipated for at least 3 years postoperatively. If there is less than 3 years of spine growth
remaining patients will typically be better treated with a definitive spinal
fusion (curves greater than 50 degrees) or other growth modulation techniques
such as vertebral body tether or posterior distraction constructs (curve 40-60
degrees).
growth remaining to justify the modulation or guidance of spine growth. In general, we perform this surgery in patients
where spinal growth is anticipated for at least 3 years postoperatively. If there is less than 3 years of spine growth
remaining patients will typically be better treated with a definitive spinal
fusion (curves greater than 50 degrees) or other growth modulation techniques
such as vertebral body tether or posterior distraction constructs (curve 40-60
degrees).
How is the amount of growth remaining estimated?
The main factor used in this determination is radiologic
evidence of the child’s “bone age”, which can be very different to their
chronologic age, based on the date of birth.
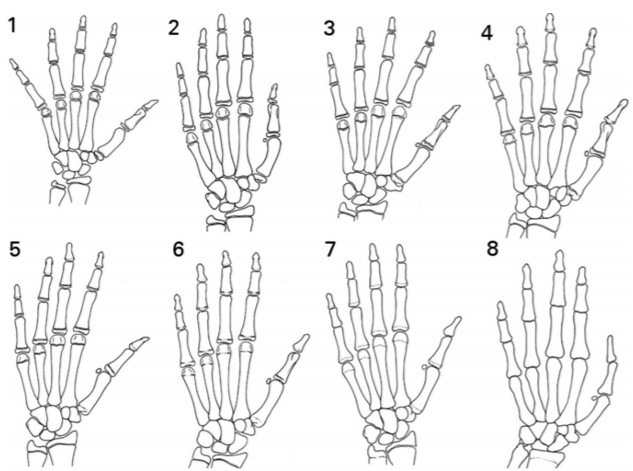
Currently the main classification used for determination of “bone age”
is the Sanders Classification (reference 1), which uses radiologic evaluation
of the growth plates in the hand. The
other method is to judge the amount of ossification (bone development) on the
top of the iliac crests (hip bone), and is called the Risser Grade.
evidence of the child’s “bone age”, which can be very different to their
chronologic age, based on the date of birth.
Currently the main classification used for determination of “bone age”
is the Sanders Classification (reference 1), which uses radiologic evaluation
of the growth plates in the hand. The
other method is to judge the amount of ossification (bone development) on the
top of the iliac crests (hip bone), and is called the Risser Grade.

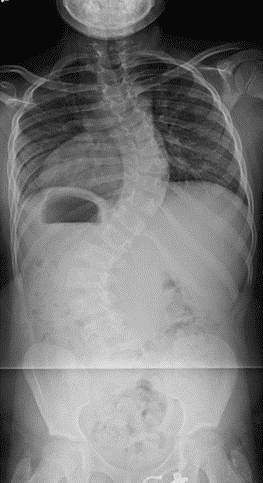
Which scoliosis curve patterns can be treated with Shilla?
The most common curve pattern treated is the single curve
patterns (thoracic or thoracolumbar), and is the easiest to manage. Double major curves (one thoracic and one
lumbar) and single lumbar curves have been treated with Shilla constructs, but
there is much less clinical experience in these curve patterns.
patterns (thoracic or thoracolumbar), and is the easiest to manage. Double major curves (one thoracic and one
lumbar) and single lumbar curves have been treated with Shilla constructs, but
there is much less clinical experience in these curve patterns.
 |
| Thoracic curve |
 |
| Double Major |
Which diagnoses have been treated with Shilla?
Diagnoses for which the Shilla has been used include:
infantile and juvenile idiopathic scoliosis, congenital scoliosis, Beale’s
syndrome, myelomeningocele, Marfan’s, neurofibromatosis, spinal muscular
atrophy, arthrogryposis, multiple pterygium syndrome, spinal cord tumors, Prune
Belly, Dandy-Walker, hypophosphatasia and dwarfism. In general, all types of early-onset scoliosis
(idiopathic, congenital, neuromuscular and syndromic) can be effectively
treated by Shilla Growth Modulation System.
infantile and juvenile idiopathic scoliosis, congenital scoliosis, Beale’s
syndrome, myelomeningocele, Marfan’s, neurofibromatosis, spinal muscular
atrophy, arthrogryposis, multiple pterygium syndrome, spinal cord tumors, Prune
Belly, Dandy-Walker, hypophosphatasia and dwarfism. In general, all types of early-onset scoliosis
(idiopathic, congenital, neuromuscular and syndromic) can be effectively
treated by Shilla Growth Modulation System.
What is the age range for patients treated with Shilla?
Ages at the time of surgery have ranged from 23 months to 11
years with the average patient being around 6-8 years.
years with the average patient being around 6-8 years.
How do you decide when to do a Shilla?
Curve magnitude, documentation of curve progression, and
skeletal age have been the key determinants in the decision to operate.
skeletal age have been the key determinants in the decision to operate.
What is the longest follow-up at Wash U?
10 years postop
What does the prototypical construct for look like?
If you look at the blog post from August 2018 I demonstrated
a common spinal construct for Shilla.
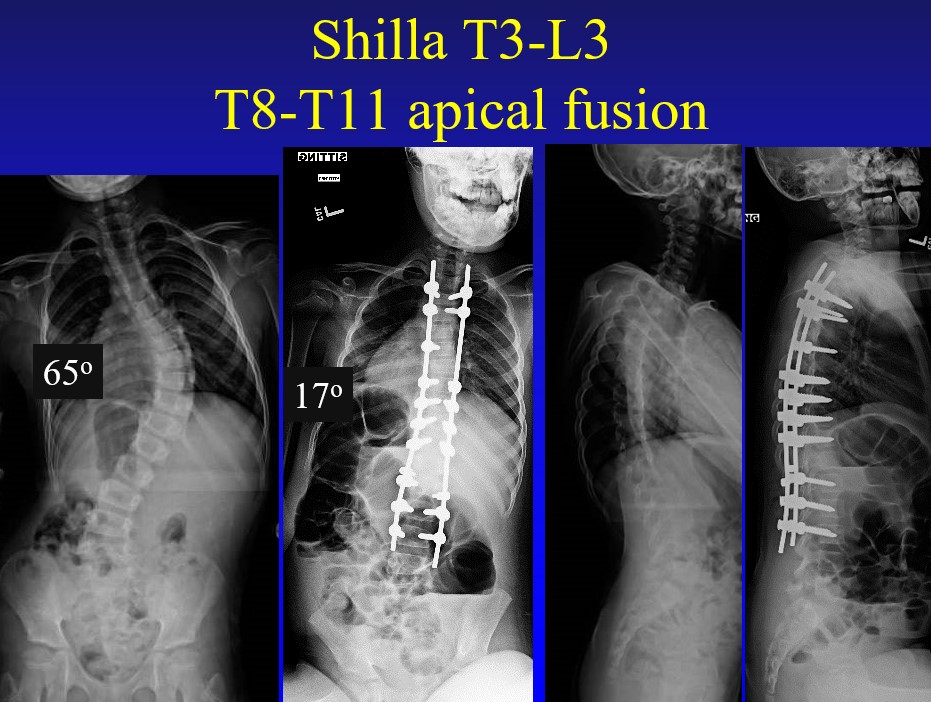
What makes Shilla different than growing rod construct is the most
curved part of the spine (called the apex) is actively straightened by using
multiple pedicle screws, and then creating a solid bony fusion. By fusing the apex of the scoliosis this most
problematic part of the spine will not curve again and will remain in a
straightened position. The apex fusion
is usually 2-4 vertebral levels, and the below case has 4 vertebral levels
fused T8 through T11, using 8 pedicle screws.
There are 5 screws above and 5 screws below the apical fusion, and these
are the Growth Guidance or Shilla screws.
These 10 screws will guide spinal growth along the straightened rods
above and below, which is why the rods are left long. As the spine grows the Growth Guidance or
Shilla screws will slide away from the middle of the construct.
a common spinal construct for Shilla.
What makes Shilla different than growing rod construct is the most
curved part of the spine (called the apex) is actively straightened by using
multiple pedicle screws, and then creating a solid bony fusion. By fusing the apex of the scoliosis this most
problematic part of the spine will not curve again and will remain in a
straightened position. The apex fusion
is usually 2-4 vertebral levels, and the below case has 4 vertebral levels
fused T8 through T11, using 8 pedicle screws.
There are 5 screws above and 5 screws below the apical fusion, and these
are the Growth Guidance or Shilla screws.
These 10 screws will guide spinal growth along the straightened rods
above and below, which is why the rods are left long. As the spine grows the Growth Guidance or
Shilla screws will slide away from the middle of the construct.
Please send me any questions you may have about this
surgical procedure….
surgical procedure….
References:
1.
Sanders JO, Khoury JG, Kishan S, Browne RH et
al. Predicting scoliosis progression from skeletal maturity: a simplified
classification during adolescence. J Bone Joint Surg Am 2008; 90(3):540
Sanders JO, Khoury JG, Kishan S, Browne RH et
al. Predicting scoliosis progression from skeletal maturity: a simplified
classification during adolescence. J Bone Joint Surg Am 2008; 90(3):540